Stripping: It’s What You Don’t See That Should Concern You
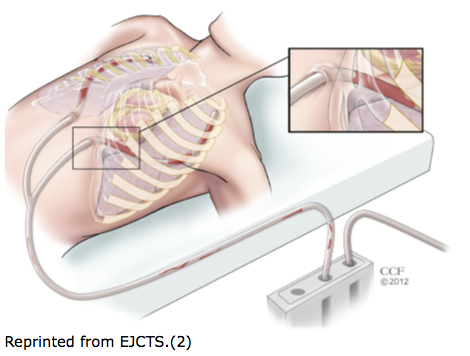
At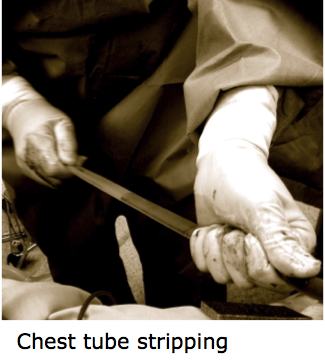 the end of every open-heart surgery, surgeons place chest tubes in the surgical spaces to evacuate any post-surgical blood and/or fluid until normal coagulation is restored and hemostasis is achieved. The goal is to evacuate as much of the blood from these spaces as possible before the chemically thinned blood undergoes the phase change from liquid to solid as the coagulation system is restored. Any blood that is not effectively evacuated will naturally turn to clot, which the body then has to break down in a process called lysis. Depending on the volume of blood clot retained, this process can cause additional clinical complications that can last for weeks or months, and is a leading cause of hospital readmission.
the end of every open-heart surgery, surgeons place chest tubes in the surgical spaces to evacuate any post-surgical blood and/or fluid until normal coagulation is restored and hemostasis is achieved. The goal is to evacuate as much of the blood from these spaces as possible before the chemically thinned blood undergoes the phase change from liquid to solid as the coagulation system is restored. Any blood that is not effectively evacuated will naturally turn to clot, which the body then has to break down in a process called lysis. Depending on the volume of blood clot retained, this process can cause additional clinical complications that can last for weeks or months, and is a leading cause of hospital readmission.
Therefore, the challenge for post-op care staff is to get the blood out before the phase change to solid clot occurs. When clots are observed in the chest tubes where they exit the skin, the obvious response is to try to get them out to keep the tubes open and flowing. For decades, nurses have used three main makeshift bedside manipulations termed tapping, milking, and stripping to try to accomplish this. Tapping and milking, generally less aggressive techniques, involve either tapping the outside of the tube or progressively squeezing the clots down the tubing. Stripping, which is done by hand or with special rollers, is done by squeezing, then pulling the length of tube through the fingers or rollers. Despite these and other techniques, a recent prospective study found that 36% of patients had chest tubes clog after heart surgery.(2)
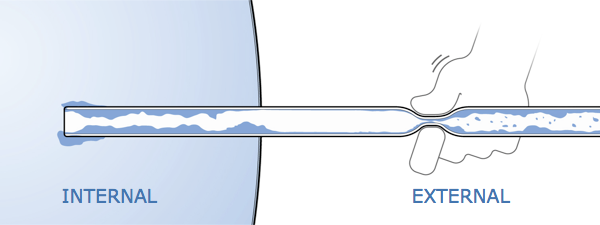
In published studies these techniques have never been shown to have any clinical benefit.(3-7) And worse, stripping has been shown to cause negative pressure bursts up to -400 cm H2O (20 times the suction pressure that is routinely applied to chest tubes after surgery) giving it the potential of causing tissue injury, and potentially re-initiating bleeding.(7) This may be why 71% of nurses surveyed report that their institutions do not allow nurses to strip chest tubes.(1)
Why don’t milking and stripping work? Probably because 86% of clogged chest tubes are clogged inside the patient and aren’t visible to clinicians.(2) By the time a nurse observes clots in the external portion of the chest tube, the portion inside the patient is most likely already obstructed, and clot is forming or has formed inside the patient. Breaking up the clots in the visible portion of the chest tube by milking and stripping won’t clear the clog inside the patient. And opening the tube and using a suction catheter to clear the clog may evacuate any leftover non-clotted blood, but the solids that have formed inside the chest are, for the most part, there to stay without significant intervention.
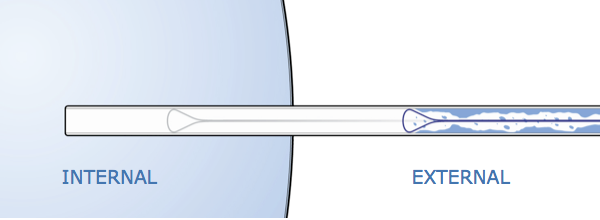 Why not be more proactive in preventing these problems? PleuraFlow ACTenables clinicians to actively clear chest tube obstructions, even those not visible externally. Combined with a systematic blood evacuation strategy, clinicians can proactively prevent chest tube clogging and maximize the evacuation of post-surgical blood.
Why not be more proactive in preventing these problems? PleuraFlow ACTenables clinicians to actively clear chest tube obstructions, even those not visible externally. Combined with a systematic blood evacuation strategy, clinicians can proactively prevent chest tube clogging and maximize the evacuation of post-surgical blood.
- Shalli S, Saeed D, Fukamachi K, Gillinov AM, Cohn WE, Perrault LP et al. Chest tube selection in cardiac and thoracic surgery: a survey of chest tube-related complications and their management. J Card Surg 2009;24: 503–9.
- Karimov JH, Gillinov A M, Schenck L, Cook M, Kosty Sweeney D, Boyle EM, Fukamachi K. Incidence of chest tube clogging after cardiac surgery: a single-centre prospective observational study. Eur J Cardiothorac Surj 2013; 1-8.
- Isaacson JJ, Brewer MJ. The effect of chest tube manipulation on mediastinal drainage. Heart and Lung 1986;15:601–605.
- Lim-Levy F, Babler SA, De Groot-Kosolcharoen J, Kosolcharoen P, Kroncke GM. Is milking and stripping chest tubes really necessary? Ann Thorac Surg 1986;42:77–80.
- Pierce JD, Piazza D, Naftel DC. Effect of two chest tube clearance protocols on drainage in patients after myocardial revascularisation surgery. Heart and Lung 1991;20:125–130.
- Wallen M, Morrison A, Gillies D, O’Riordan E, Bridge C, Stoddart F. Mediastinal chest drain clearance for cardiac surgery. Cochrane Data- base of Systematic Reviews 2002.
- Duncan C, Erickson R. Pressures associated with chest tube stripping. Heart and Lung 1982;11:166–171.