What’s your Protocol?

Proactive Protocols to Reduce Complications After Cardiac Surgery
Improving outcomes and reducing costs is a continual effort in modern healthcare. For heart surgery patients, a good place to start is by focusing on something that is common to nearly all patients recovering. All cardiac surgery patients have some degree of bleeding postoperatively, and chest tubes are used to evacuate this blood from the pleural and/or pericardial spaces. Studies have shown that higher chest tube output is statistically associated with longer ICU stays, more complications, higher costs, and a greater risk of mortality. (1, 2)
The tipping point in terms of patient outcomes occurs early in the recovery period, within the first six hours postoperatively, and when total chest tube output exceeds 200mL in any one-hour period. (1) A part of the problem may not be what is evacuated, but what is not evacuated. (2) Chest tube clogging, which has been found to occur in 36% of heart surgery patients, can cause blood to be retained around the heart and lungs, which can lead to Retained Blood Complex (RBC). (3) Chest tube clogging is also statistically associated with more complications, including atrial fibrillation. (3)
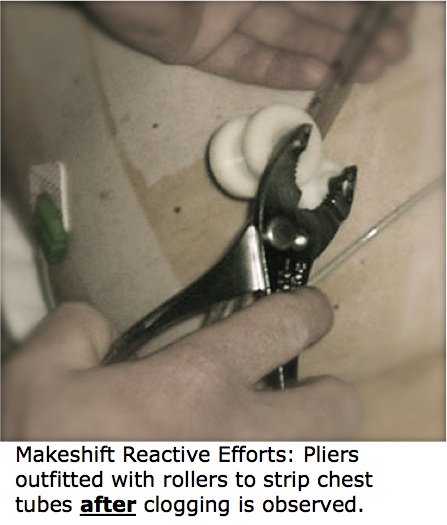
The link between outcomes and postoperative bleeding has led many hospitals to look at their postoperative evacuation management protocols. Nurses in the postoperative ICU, among many other things, monitor chest tube output, check for indications that the tubes are obstructed, and notify the physicians if chest tube output suddenly ceases or reaches an alarming level. In the absence of defined tube management protocols to address chest tube clogging, however, clinicians use makeshift methods like milking, tapping, stripping, and open suction. These approaches are all reactive, and none have been shown to have clinical benefit. (4-6) By the time clot is visualized in the chest tubes, the evacuation has often been impaired for some time, allowing blood and clot to accumulate in the pleural and/or pericardial spaces.
Proactive clearance with PleuraFlow ACT, however, has been shown to be clinically efficient, to improve the evacuation of post-surgical blood, and to reduce the volume of blood retained in the surgical spaces. (7-9) With PleuraFlow ACT, the only FDA cleared chest tube clearance system, hospitals are now developing chest tube clearance protocols to proactively prevent chest tube clogging. By actively and systematically maintaining chest tube patency, top hospitals are working to improve the efficiency of chest tube management, and potentially decrease incidence of RBC complications by reducing the volume of retained post-surgical blood.
For more information about how the PROACT program and PleuraFlow ACT can help your facility address this common and costly problem, contact us.
- Dixon, B., Santamaria, J.D., Reid, D., Collins, M., Rechnitzer, T., Newcomb, A.E., Nixon, I., Yii, M., Rosalion, A., and Campbell, D.J. 2012. The association of blood transfusion with mortality after cardiac surgery: cause or confounding? Transfusion.
- Christensen, M.C., Dziewior, F., Kempel, A., and von Heymann, C. 2012. Increased chest tube drainage is independently associated with adverse outcome after cardiac surgery. J Cardiothorac Vasc Anesth 26:46-51.
- Karimov JH, Gillinov A M, Schenck L, Cook M, Kosty Sweeney D, Boyle EM, Fukamachi K. Incidence of chest tube clogging after cardiac surgery: a single-centre prospective observational study. Eur J Cardiothorac Surj 2013; 1-8.
- Wallen M, Morrison A, Gillies D, O’Riordan E, Bridge C, Stoddart F. Mediastinal chest drain clearance for cardiac surgery. Cochrane Data- base of Systematic Reviews 2002.
- Pierce JD, Piazza D, Naftel DC. Effect of two chest tube clearance protocols on drainage in patients after myocardial revascularisation surgery. Heart and Lung 1991;20:125–130.
- Isaacson JJ, Brewer MJ. The effect of chest tube manipulation on mediastinal drainage. Heart and Lung 1986;15:601–605
- Shiose, A.; Takaseya, T.; Fumoto, H.; Arakawa, Y.; Horai, T.; Boyle, E. M.; Gillinov, A. M.; Fukamachi, K. “Improved drainage with active chest tube clearance.” Interactive CardioVascular and Thoracic Surgery 10 (5): 685–688.
- Arakawa, Yoko; Shiose, Akira; Takaseya, Tohru; Fumoto, Hideyuki; Kim, Hyun-Il; Boyle, Edward M.; Gillinov, A. Marc; Fukamachi, Kiyotaka. “Superior Chest Drainage With an Active Tube Clearance System: Evaluation of a Downsized Chest Tube.” The Annals of Thoracic Surgery 91 (2): 580–583.
- Perrault, Louis, Michel Pellerin, Michel Carrier, Raymond Cartier, Denis Bouchard, Philippe Demers, Edward M. Boyle. The PleuraFlow Active Chest Tube Clearance System: Initial Clinical Experience in Adult Cardiac Surgery. Innovations. 2012;7:354-358.